
Thanopoulou, K. (2025). Connections and Separations: From the Individual to the Family and from the Family to the Individual [JD]. Systemic Thinking & Psychotherapy, 26, 14–27. https://doi.org/10.82070/syst20252605
This paper is based on a lecture given at a conference held in October 2024 to celebrate the 30 years of operation of the Family Therapy Unit of the Attica Psychiatric Hospital, and a farewell to the founders of the Unit.
Abstract
In this paper, on the occasion of the Family Therapy Unit's Conference "Celebrating our 30 years", we discuss connection, separation and early termination as part of the therapeutic process. An important aspect is the unique qualities of psychotherapy when it occurs in the public sector with all the impersonal, undifferentiated and archaic connotations it carries as an institution, which permeate and influence the relationships of those working within it, and should certainly be processed and reflected upon. Reference is made to the complexity of psychic work with the family, the aim of which is the 'empty nest' phase. At the end of this paper, emphasis is placed on saying goodbye to the people who conceived and created the Unit.
Key words: connection, separation, therapeutic process, premature terminations, public sector, family therapy, empty nest, our personal goodbyes.
"There is no 'I' without 'You.'" Buber
Our life’s journey is marked by the endeavour to embrace living with others, while being able to bear the pain of their absence. The therapeutic process, like life itself, holds within it the delicate art of forging connections and the poignant art of saying goodbye.
The initial connection is the act of welcoming and creating that safe space, as described in Bowlby’s theory, which allows for the exploration of the inner world and the relationships of our clients. The relationship we build becomes the cornerstone of psychotherapy - a bond where our presence must make room for our absence as well. Not so close that clients feel burdened or constrained, yet not so distant that they feel lost or abandoned - just close enough to meet their genuine need (Balint, 1986).
The therapeutic encounter is a living, human experience within which various events unfold and emotions arise, that require reflection and processing by both parties. This encounter needs to encompass all the contradictions, and the confusing and unpredictable elements that may accompany relationships, growth, transitions, separations, and the journey toward individuation. Under these conditions, the therapeutic relationship can act as a developmental catalyst, activating psychological processes that had previously been inhibited (for more information see Thanopoulou, 2013).
The therapeutic journey, winding through labyrinthine paths, hesitations, struggles, adventures, and revelations, inevitably leads to its conclusion - the farewell. Like any loss, the end of therapy stirs conflicting emotions in both clients and therapists. The client often wrestles with balancing the need for autonomy and freedom against the anxiety of losing the intimacy and security that the therapeutic process represents (Holmes, 2001). As Worden reminds us, without the psyche's capacity to endure the sorrow of separation and return to a fundamental internal organization oriented toward life, survival would be exceedingly difficult (Worden, 2009). Separation becomes possible when both intimacy and autonomy have been achieved. In reality, much like parenthood, the goal of therapy is for the client to be able to step fully into their life without the therapist’s accompaniment - to have succeeded in becoming their own parent.
Pedder (1988) suggests that the end of therapy resembles the psychological state of an adolescent preparing to leave home, navigating various phases between “inside” and “outside” before achieving autonomy. Similarly, the therapist must remain aware of their own emotions, and tolerate the client’s emotional oscillations between engagement and disengagement as they negotiate the termination of the therapeutic process. According to Holmes (2001), there is a constant dialectic in psychotherapy, as in life, between closeness and separation, attunement and challenge, attachment and loss. The end is always present, casting its shadow over therapy from the very beginning, and when it finally arrives, it serves as the culmination of countless smaller endings that have preceded it - such as separation anxiety triggered by the conclusion of a session, breaks for holidays, or even subtle enactments like being late or forgetting an appointment. In reality, based on our experience, clients in the final phase of therapy often do not want to leave. They receive care and have done all the hard, painstaking work, yet they recognize that a cycle has come to an end. In their own rhythm, they bid us farewell.
We often encounter premature terminations or interruptions in therapy. The reasons can be numerous - dissatisfaction with the therapist’s approach, with the therapist themselves (lack of rapport, trust, or a sense of incompatibility, etc.). At times, painful emotions or sensitive issues from their personal history arise during therapy, making it difficult for clients to manage, commit to, or process them further. Thus, they leave because that is as far as they were able to go. As therapists, we encourage them to come and discuss their decision to end therapy, but this is not always accepted, and we must respect their decision.
At times, clients unconsciously repeat in therapy what they fear most in their lives - abandonment. Bowlby (as cited in Holmes, 2009) reminds us that the ability to manage loss and separation, with the accompanying anger, sadness, and reconciliation, is linked to secure attachment. Many of our clients come with unresolved emotional issues and patterns of insecure relationships that they tend to repeat with us. Very often, they may abandon therapy when their core beliefs are challenged. Similarly, some families leave when they are threatened with shedding their armour and revealing their most vulnerable sides. Other times, an obstacle to the therapeutic process arises through triangulation. In our clinical practice, we encounter families that function in a triangulating way with mental health structures. Without committing themselves, and without allowing other members to form personal relationships with the therapist, they involve - triangulate - many different mental health professionals, temporarily relieving their anxiety and tensions, yet remaining impenetrable in terms of their internal world, replicating their chaos outside the boundaries of the family system.
The opportunity for repairing relationships is not always successful, and it is important for us to be open and reflective regarding our own responsibility in this process. How do we contribute, or how can we facilitate the repair, and prevent repetition? According to Cecchin and his colleagues, when a therapist begins to reflect on the impact of their stance and assumptions, they take on both an ethical and a therapeutic position (Cecchin et al., 1992). However, we must always keep in mind the popular joke: how many psychologists does it take to change a lightbulb? (One, as long as the lightbulb is willing to change).
In the literature, we also find positive reasons for the termination of therapy. Some clients leave because they have made satisfactory progress on the issues that initially brought them to therapy. The issue, however, is that for various reasons, they avoid saying goodbye, as if they are keeping a potential door open for future use, which, in most cases, never happens, except in rare instances. As Zachariades (2015) writes, "We have neither learned to love nor to hate separation. It remains unmanageable, in the form of a fear".
Premature terminations often stir feelings of failure or rejection, especially – but not exclusively - in younger colleagues, perhaps because they activate their own attachment systems or even their omnipotent expectations for therapy. It is important to remember that the amount of therapy people want does not necessarily align with the amount of therapy we want for them.
The inherent ambivalence of the end tests our ability as therapists to tolerate the ambivalence and uncertainty that exists within the therapeutic journey, to face both the satisfaction, joy, and sadness in the face of loss, and to maintain a realistic appreciation of our own strengths and weaknesses, as well as those of our clients. It is crucial to accept our clients' self-organizing capacity, to respect their pace, endurance, and limitations, without losing faith in the process of psychotherapy - a process of exploration that is open to what we are and to what we are becoming. It is a path of opening and expanding our choices; a path that unfolds further with each step one takes.
We could even say that the power of psychotherapy lies precisely in its ability to not confirm the client's traumatic relational script, but rather to offer, through the relationship that will be built with the therapist, new possibilities for processing, thinking, and experiencing the events of their life, and consequently, the narrative they will create for their own history. A narrative that, as it gains structure and coherence, allows the therapist to step away from the role of the autobiographical assistant, with the client themselves now assuming that role.
Therapy, however, never operates as we imagine or as our textbooks may teach us, since it is a process that takes place within an emerging set of relationships and patterns, which may either function and lead to change, or work partially, or not at all. Moreover, we recognize that every therapeutic process retains an enigmatic dimension, unknown to the participants in the therapeutic relationship. In any case, it is accepted that it is not the therapist alone, nor the client alone, but the client and the therapist together that form the vehicle of transformation and growth.
An important factor is also the particularity of psychotherapy when it takes place in the public sector, with all the impersonal, undifferentiated, and archaic aspects it carries as an institution, especially when it concerns a psychiatric hospital; these elements permeate and influence the relationships of those working within it, and they certainly need to be processed and reflected upon.
Charalabaki (2017) writes: “What is the role of a therapist in the public sector? To what extent can issues of autonomy and development be promoted through psychotherapeutic work by a therapist who personally experiences a lack of autonomy, who is often involved in boundary-less relationships, and has a diminished ability to take full individual therapeutic responsibility? How can emancipation be the goal of a therapist who, within their working environment, does not feel emancipated?” (Charalabaki, 2017, p. 146).
Finding cracks and passages within the constraints of the public sector, using creativity and flexibility, means emerging, each time in different conditions, as a therapist/person, with one’s own dilemmas and questions. According to Ceccchin and his colleagues (2009), one way to survive among the many conflicting messages inherent in both institutional structures and outpatient care settings is to adopt an attitude of irreverence. This concept protects the therapist from becoming stuck in the dominant ideology of their scientific model or the framework in which they work, and encourages them to stay vigilant to the genuine needs of their clients, offering them alternative perspectives and meanings.
Families.
"All happy families are alike; each unhappy family however, is unhappy in its own way" - Leo Tolstoy
Clinical Vignette: «Everything one could ask for»
The parents, both 38 years old, attend their first session with their 9-year-old daughter following a recommendation from the school’s social worker. They do not seem to have a clear request of their own. They mention that they had almost forgotten the appointment, the father remembered it the day before, so they eventually came. The mother is overweight, somewhat loud, speaks more than the father, and could be described as impulsive. The father appears more subdued. They report that the problem is that their daughter constantly demands their attention. The mother comments that it irritates her because their daughter has grown up and is no longer a baby. The father adds that she insists on having her way. If she does not get what she wants, she reacts by shouting. Both parents agree that she is never satisfied with anything.
They then mention, in a rather detached manner, that their daughter has a very serious illness, cystic fibrosis. The diagnosis was made when she was only two months old, and the disease proved to be disruptive for their relationship as a couple. The mother became angry with the father, and they separated. As she disarmingly admitted, “I saw the hereditary nature of the illness in my husband and felt angry with him. Who else could I possibly blame? Myself?” Following their daughter’s diagnosis, the mother initially fell into depression, and later became romantically involved with someone who had many personal issues. Although separated, the couple continued living together until their daughter turned four. During this period, the mother was physically and emotionally unavailable to her daughter, frequently coming and going. Once the mother recovered, they moved into different houses.
Now, the mother is seeking to make up for lost time with her daughter. The father, on the other hand, seems to have stepped in to compensate for the mother’s absence. In both homes, their daughter still sleeps in the same bed as her parents. The mother says she will let her leave on her own when the daughter feels ready. She doesn’t want, as she notes, her daughter to feel pressured into anything. The mother adds that she herself enjoys her daughter’s cuddles, while for the father, their daughter serves as a kind of companion (almost as though compensating for the loss of his wife). Both parents also admit, as if it were the most normal thing, that their daughter still uses a pacifier. Other than that, the child is described as being very independent when it comes to her studies and responsibilities.
The girl seems serious, composed, thoughtful, and faintly melancholic - or is it perhaps my own sadness projected onto her? She appears to bear the burden of both her illness and her parents on her young shoulders. The father shares that she has questions and worries about her illness - whether she will overcome it, whether she will one day have her own family and children. Her concerns sound completely reasonable, yet the parents appear to settle for saying that she is regularly monitored by doctors and is doing quite well.
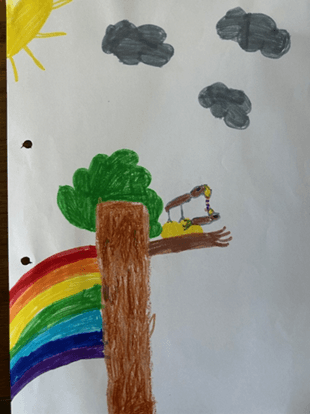
I ask the girl to draw a bird's nest (a projective test). She goes to an adjacent children's table in the consulting room, and as she goes to sit on the children's chair she wonders aloud whether it will hold her or break. Eventually she sits down and draws. We discuss her drawing. A bird gives her child a worm. It is raining, it is cloudy and then the sun comes out and the mom or dad is looking for food for their child and brings it to it. Title of the painting: "Everything one could ask for".
I feel shocked by the enmeshment of this family. There is an abundance of everything - there is no absence, no separation. Words intertwine: pacifier, bed, baby, illness, young, old, gained time, lost time, compensation. I share with them the paradox of the girl being too old to be seeking attention, but too young to let go of her parents’ bed and her pacifier. Who is young, and who is old? What are they avoiding by keeping their child a baby? What is the greatest fear in this family? Is it the fear of death, or the fear of their child growing up, which stirs their own fear of death? Are they keeping her a baby to shield themselves from their own anxieties about death? Let us not forget that cystic fibrosis is the most common hereditary disease with poor prognosis among the Caucasian population.
Undeniably, physical illness brings unbearable pain to the entire family. How can the unspoken, the incomprehensible, that which the human mind cannot bear to think even of be contained? Yet, an illness is not the entirety of a child’s identity. Even if this child may one day die, she still has the right to be supported by her parents to grow and maintain a quality of life.
How can the therapist introduce reality in tolerable doses - not extreme or traumatic ones? How can the therapist impose a prohibition (e.g., "At this age, your child cannot sleep in your bed or use a pacifier") while simultaneously maintaining a non-directive stance that allows space for thought and exploration?
How can the therapist avoid imposing their own values and beliefs while also not becoming absorbed into the family system, losing their position and role?
The emphasis in the Family Therapy Unit is on working with families - a deep dive into the unspoken, contradictory, and unrefined aspects of family relationships, and simultaneously a journey into the unpredictable and adventurous nature of relationships and the enigma of human nature.
But what about families? Why do we often avoid working with families? This becomes even more evident in the private practices of colleagues who primarily work with individuals and groups.
A first observation is that we all carry our family within our memory. Our childhood years reside within it. To paraphrase Winnicott’s “home is where we start from”, family is the place from which we begin. It is within the family that we grow and learn about ourselves and our relationships. Family relationships can strengthen us, but they can also wound us. Therefore, working with families can ignite our own emotional knots or blind spots. As McGoldrick (1992, p. 20) observed: "I have the strong impression that one tends to get stuck in family therapy in the same ways one gets stuck in one’s own family". Similarly, Bowen (1978, p. 468) noted that the family therapist often faces similar challenges in their own family to those encountered in the families they work with professionally, and that they bear a responsibility to define their role within their own family if they wish to function adequately in their professional practice.
According to Byng-Hall (2002; 2008), many therapists were parentified children in their families of origin. It is important for them to understand how this influences their work with families, as it offers them insight into the strengths as well as the challenges faced by parentified children. This awareness becomes especially significant when they feel themselves being drawn more into a parental role and less into a therapeutic role with the families they work with. Byng-Hall himself suggests that he is often overly protective and positive towards family members, while being hesitant to confront or challenge them.
But families often avoid us as well, since seeking help requires them to challenge their often deeply ingrained belief that "what happens at home stays at home". Quite frequently, they send their children to therapy at specialized centres to address their symptoms, ignoring their own crucial role in resolving those symptoms. Unfortunately, this practice is sometimes reinforced by the centres themselves and certain professionals.
Another important observation is that families “struggle” and create challenges for us, not only because they carry personal traumas from their own families of origin, but also because they absorb all the shockwaves of the social landscape. As Katia Charalabaki (2017) aptly noted, elements of distortion within the social value system penetrate family relationships under conditions of societal pressure, shaping their dynamics.
We can imagine how the successive crises of recent years, as well as the emergence of the pandemic, created an uncertain, unstable, and fluid environment that significantly affected the mental and daily lives of families. Reality invaded therapy in a cataclysmic and traumatic manner, complicating mental processing, symbolization, and the search for meaning. I will not elaborate further on this, as it has been thoroughly analyzed by Katia Charalabaki in her excellent book Families in Troubled Times (2027).
Working with families is a complex, multifaceted, and demanding psychological endeavour. The multiplicity and intricacy of interactions add greater complexity for the therapist.
It is no coincidence that, in family therapy, the use of a one-way mirror and subsequently a reflective team serves as a source of multiple perspectives or voices, aiming to encompass the complexity of family dynamics.
According to Gerson (2015), the family therapist discovers a framework within which the family is embedded. It is real, present, and produces consequences. It unfolds before us, and often sweeps us away like a giant wave. This is not merely the narrative of the client, as is the case in individual therapy. These are living relationships, tangible and embodied. Family members speak, confront, argue, insult, attack, resist, conceal, hide, remain silent, and protect one another. The consulting room becomes the stage where countless emotionally charged scenarios are enacted, revolving around issues of dependence, autonomy, loyalty, betrayal, belonging, freedom, closeness, distance, love, hate, acceptance, and rejection.
For the therapist, balance becomes even more challenging. A therapeutic stance of "equal distance" or "equal closeness" to all family members is required - one that avoids blaming, but assigns responsibility for the co-creation of a dysfunctional relational network to all. As Sakkas has written, in such a situation, everyone becomes simultaneously a "victim", a "perpetrator", and a "saviour" (Sakkas, 2016).
The family is our first collective identity - the initial "we" from which the "I" will emerge. Parents undertake a challenging, almost impossible profession, as Freud put it: raising and educating their children. In turn, children educate their parents by confronting them with unresolved and unprocessed issues from their own past. The process of giving birth to and raising a child (and simultaneously becoming a parent - let us recall Daniel Stern’s The Birth of a Mother) - represents a moment when the past, present, and future converge.
According to Holmes (2009, pp. 276–277), "The family therapy perspective shows how attachment patterns perpetuate themselves through the life cycle, event scripts being the psychological equivalent of the genome [...] The basic aims of psychotherapy – the need to provide a secure base, to help people express and come to terms with anger and disappointment (both of which can be seen in terms of separation protest), to achieve integration and coherence within themselves and their families – represent an attempt to intervene in this cycle, altering not so much an individual personality as a pattern of relating so that good experiences lead, by benign rather than vicious circles, to yet more good experiences, and so on".
Through our relationship with our children, our own history is reactivated. Our early experiences shape us, even though they often escape our conscious memory. However, they are inscribed in our emotional legacy, which is transmitted in subtle, often unspoken ways from one generation to the next. When this transmitted history fosters autonomy and growth, it ensures continuity for future generations. Conversely, when parents pass on unresolved and unprocessed traumas from their personal histories, subsequent generations inevitably bear the burden, and the trauma is perpetuated.
Understanding that one is the product of a history allows them to gain a sense of personal engagement with life and the shaping of their own narrative. As Goethe said: "What you inherit from your ancestors, take it and make it your own to truly possess it" (for more information see Thanopoulou 2025, in print)
And I believe this is where our intervention becomes particularly significant.
Leaving Home - Separations
"And so we live, constantly saying farewell".
Rainer Maria Rilke
I am at the airport, watching two parents bid an emotional farewell to their son, who, as far as I can tell, is leaving to study. I find myself transfixed, observing them. This moment, as they part with their child, feels so unique and sacred. The mother is visibly tearful, while the father struggles - but seemingly fails - to hold back his own tears. The son appears awkward and bewildered, caught between what he is leaving behind and what lies ahead. I reflect on how many families, consciously or unconsciously, resist experiencing such painful but vitally necessary moments of separation. Instead, they come to therapists carrying symptoms and dysfunctions in a desperate attempt to avoid the anguish of loss and of bidding farewell.
Whitaker once said that family therapy begins like a blind date and ends with an "empty nest". We can all agree that parenting is a delicate balance between involvement and letting go. The lifelong process of "being there so you can be left behind" is one of the most challenging and threatening aspects of parenthood. This is the moment of the "speaking back", as poetically described by Rhea Vitali, referring to the era of farewells from our children. Psychoanalyst Meropi Michaleli likens children to migratory birds: parents raise them, care for them, and eventually release them to the universe (as noted in an article by L. Giannarou in Kathimerini, 15/11/24). The departure of children from the family home is a pivotal moment in the family's evolution, often leading to a crisis. It is a transitional phase in which parents must manage their anxiety over separating from their child, endure the grief and loss of their parental role, and renegotiate their own relationship. The growing-up of children signifies proof of continuity for the parents, but it also brings the painful realization of the passage of time. Winnicott believed that, in the unconscious fantasy, growing up is inherently an aggressive act because "to grow up" means to take the place of one's parents (Winnicott, 1971).
The adolescent, during the leaving home stage, is tasked with renegotiating the transition from life within the family to life in the broader world. This process requires challenging parental models in order to break free from childhood roles and dependencies, and differentiate from their family of origin, and establish their own identity - without, however, severing ties with their parents. As Winnicott aptly put it, the eternal task of humanity is "to remain separate yet connected".
As Bowlby wisely observed (1979), "It is easier to leave without things going wrong if we are securely attached to our parents than if we are anxious about them or in conflict with them".
Our Own Goodbyes
“...If we forget,
The wind will take us away,
The wind will take us away…”
Forough Farrokhzad
Finally, I could not help but turn the focus to our own goodbyes today. As Katia Charalabaki (2018, p.15) wrote, “An anniversary is always a moment that unites, brings joy, and creates new expectations for the future. Not one to forget the difficulties, and idealize, in a utopical manner, the history through a narcissistic presentation of it, but because, ultimately, an anniversary is the historical reminder that a system remained open and alive, and did not sink into the underground currents of entropy". However, today’s anniversary, apart from the celebration of meeting and the creative journey of 30 years, also involves the farewell of the people who conceived and created the Unit. This is something that saddens us but also entrusts us with the responsibility of continuity.
Every end, every farewell, makes space for something else to begin, to be born. We hope to continue. It is not entirely up to us, especially in these socio-political conditions.
I feel fortunate to have participated and still be part of a mental health facility that managed to create a crack in the mental health system and provide psychotherapy and training free of charge.
I want to thank Katia and Fotis for giving me the opportunity to grow and evolve my professional self in an environment of freedom, respect, and vision. The path was not always easy. The confrontations and disagreements were inevitable, but also extremely beneficial. Always in a manner that provoked thought.
I want to thank Soula Kati for everything we shared and endured. I admit I feel lonelier without her presence, although I enjoy working with Georgia Moschakou and Ioanna Papaioannou, Nikos Marketos who trusts us, Ioanna Anagnostopoulou who organizes us, Katerina Kostakopoulou who takes care of us in her unique way, and Eleni who cares of our working environment. Finally, I want to apologize to Ersi Tsopanaki and Maria Stathaki, who joined the Unit at a difficult time, when it was bidding farewell, and perhaps somewhat wavering between the old and the new. We did not welcome them with the joy they deserved. Lastly, I want to thank from the bottom of my heart all the clients who entrust us with their stories.
References
Balint, M.(1986). The unobtrusive analyst. In Kohun, G. (ed.), The British School of Psychoanalysis. London Free Associations.
Bowen, M. (1978). On the differentiation of self. In Family Therapy in Clinical Practice. New York: Jason Aronson, pp. 467–528.
Bowlby, J. (1979). Self-reliance and conditions that promote it. In The Making and Breaking of Affectional Bonds. London: Tavistock Publications.
Byng-Hall, J. (2002). Relieving parentified children’s burdens in families with insecure attachment patterns. Family Process, 41, 375–388.
Byng-Hall, J. (2008). The crucial roles of attachment in family therapy. Journal of Family Therapy, 30: 129-146.
Cecchin, G. Lane, G. Ray, W. (2009). Ασέβεια: Μια στρατηγική επιβίωσης για θεραπευτές . Θεσσαλονίκη: University Studio Press.
Γιάνναρου, Λ. (2024, Νοέμβριος 15). Πως γινόμαστε ή δεν γινόματε γονείς Η Καθημερινή. https://www.kathimerini.gr/
Γκέρσον, Μ. Τ. (2015). Ο πλαισιωμένος εαυτός . Αθήνα: Καστανιώτης.
Ζαχαριάδης, Τ. (2015). Συντροφικότητα- Αποχωρισμός. Αθήνα: Αρμός.
Θανοπούλου, Κ. (2013). Ο δεσμός και το νόημα ως αντίδοτα στο τραύμα. Η συμβολή της θεωρίας της συναισθηματικής πρόσδεσης στη θεραπεία ενηλίκων που έχουν βιώσει τραυματικές εμπειρίες. Συστημική Σκέψη και Ψυχοθεραπεία, 3.https://hestafta.org/systimiki-skepsi-psychotherapeia-periodiko/teuxos-3/desmos-noima-os-antidota-sto-trauma-synaisthimatiki-prosdesi-sti-therapeia-enilikon-me-traumatikes-empeiries.
Θανοπούλου, Κ. (2025). Ψυχικές Διαδρομές του Πένθους. Ιστορίες Απώλειας . Αθήνα: Πεδίο (υπό έκδοση).
Haley, J. (1980). Leaving Home: The Therapy of Disturbed Young People. New York: McGraw-Hill.
Holmes, J. (2001). The Search for the Secure Base: Attachment theory and psychotherapy. East Sussex, UK & Philadelphia, PA: Brunner-Routledge.
Holmes, J. (2009). O John Bowlby & η θεωρία του δεσμού. Αθήνα: Ελληνικά Γράμματα.
ΜcGoldrick (1992). Through the Looking Glass: Supervision of a Trainee’s “Trigger” Family. In J. Bing Hall and R. Whiffen, (eds.), Family Therapy Supervision. London: Academic Press.
Pedder, J. (1988). Termination reconsidered. International Journal of Psychoanalysis, 69, 495-505.
Sakkas D., (2016). "Utilising Greek Myth as a Μetaphor in the Educational Programme", in IN.PS.Y. (Institute for Children's Mental Health).
Winnicott, D. (2013). Σύγχρονες Έννοιες για την Ανάπτυξη του Εφήβου και οι Επιπτώσεις τους στην Εκπαίδευση. Στο Γ . Στεφανάτος (επιμ.) Ψυχανάλυση και εφηβεία. Κλινικά και θεωρητικά ορόσημα . Αθήνα: Εστία.
Worden, J.W. (2009). Grief Counselling and Grief Therapy: A handbook for the mental health practitioner (4th ed.). New York: Springer Publishing Company.
Χαραλαμπάκη, Κ. (2017). Οικογένειες σε δίσεκτα χρόνια. Σημειώσεις μιας ψυχιάτρου. Αθήνα : Καστανιώτης.
Χαραλαμπάκη, Κ. (2018). Αντί εισαγωγής: Τι παραμένει, Τι άλλαξε. Στο Κ. Χαραλαμπάκη, Μ. Borcsa & Κ. Θανοπούλου (Επιμ.), Αναμνήσεις και αναστοχασμοί. Ιστορίες συστημικής Ψυχοθεραπείας. Αθήνα: Εκδόσεις Κοροντζή.
